
Recently I was told I needed to go to the Youtube channel of Dr Sam BaileyA and watch one of her videosB. So I did.
This particular video is called The Truth About Virus Isolation, and yes it’s on Youtube, and no I’m not linking directly because I refuse to link to such a misleading channel. It’s ostensibly about the (lack of) isolation of the SARS-Cov-2 virus. Given that there have been a lot of papers published on this very topic, one might expect a discussion of what Bailey sees as their flaws – especially given her lead-in claim that “the scientific literature is a mess” – and at the very least reference to some of them. One would be mistaken. There is, however, a certain amount of shadeC: “I’m not sure if many virologists and scientists are aware of what they’re doing any moreD,” she says, about 10 minutes in. (For some reason she expects journalists to know more & to “call the researchers out.”)
Remember that covid-19 was first identified as a distinct infection back in December 2019 (hence the name) & SARS-Cov-2 (the virus itself) was officially named in early February 2020. The viral genome was described – and shared globally – a little earlier, in mid-January that year. And there have been a large number of papers describing isolation and genomic sequencing from patients the world over (for some examples see here, here, here & here). And here’s a detailed description of steps taken to grow & isolate the virus. Basically researchers can take the liquid that cells grow in, centrifuge it, and pass what they get through a filter.
Sam Bailey seems very hung up on dictionary definitions of “isolate” and “isolation”, but nowhere does she really look at what this entails when it comes to viruses, which (as she correctly notes) have to be grown in living tissues. In effect, this means that Koch’s Postulates can’t be applied in their entirely to viruses, which is hardly surprising since the existence of viruses hadn’t been discovered at the time that Koch developed his guidelines. In fact, even in his lifetime Koch knew that the postulates didn’t apply universally – he knew that Vibrio cholerae was found in healthy people as well as those ill with cholera, for example. In the same vein, the leprosy bacterium has so far been impossible to culture outside of living organisms (humans, armadillos – & mice’s footpads). Since then, microbiologists have adapted his original postulates to accommodate the fact that viruses cannot be grown in pure culture outside of living cells (see here, and here, as examples). Siouxsie Wiles had a bit to say about this late last year.
Bailey then moves on to statements by Vincent Racaniello (of Virology Blog), prefacing them by saying that “My opinions on what are termed viruses and how these relate to disease differ sharply from Professor RacanielloE,” and talks of “establishment virology theories.” While she includes a couple of slides with quotes that come from a video or videos by Racaniello, there are no links to the actual sources, which really made me wonder about the potential for cherry-picking in her claims regarding the lack of clarity in relevant terminology. Fortunately videos of his virology lectures are up on line, and this the one that Bailey appears to be using the most in her own video. It’s fairly easy to follow and you can hear for yourself how he defines the relevant terminology.
Just over 6 minutes into the talk, Bailey talks about “the purported virusF” before going on to show an image from a “studyG” that shows responses from some authors (far from all of them) of papers describing isolation of the virus. Again, she seems to think that without electron microscope images of virions, there has been no purification. It’s worth noting that, once the genome sequence was available and specific PCR tests developed, there was hardly a need for everyone to purify their sample and photograph it; the molecular technologies alone could confirm presence or absence of the virus. However, at the 6:24 timestamp, she complains that “they” haven’t got a “purified form” before returning to a dictionary definition for the purification of bacteria, not viruses. In any case this complaint is groundless, given that institutions such as the CDC hold reference samples of the virus. Pure virus samples are fairly straightforward to isolate from the cells in which they’re been grown. And in fact, it would have been impossible for researchers to undertake this work on the in situ structural analysis of the viral ‘spike’ protein if they didn’t first have a purified sample – in situ means in place on the viral particle. The paper even includes a description of how the pure sample was obtained.
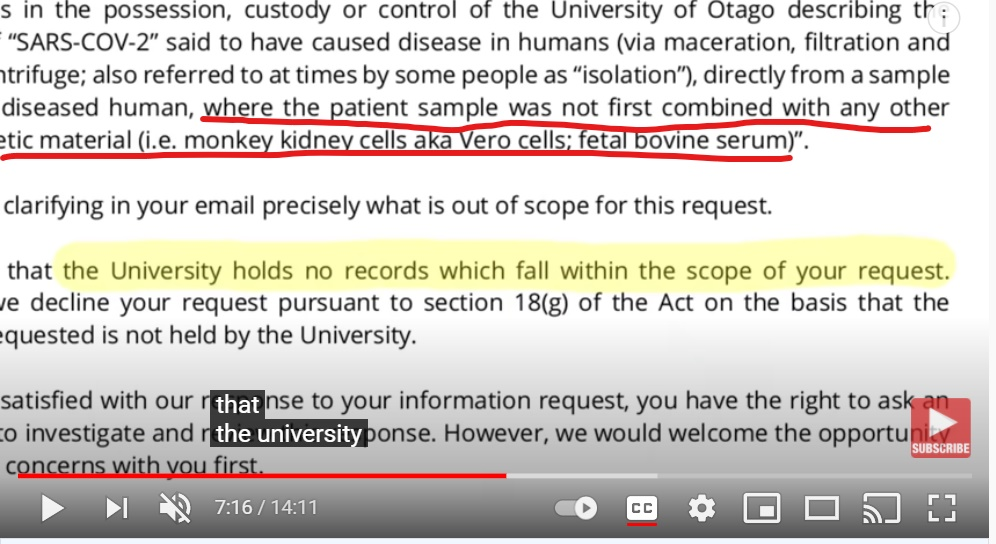
She then presents the results of a request under the Official Information Act to the University of Otago that is so carefully phrased as to suggest that those making the request wanted a negative result. Unsurprisingly that’s what they got. However, it’s clear that Otago researchers led by Prof Quiñones-Mateu & postdoctoral fellow Dr Harfoot are indeed working with the SARS-Cov-2 virus. Why the apparent discrepancy? Because, as we already know, in order to get enough virus to isolate in meaningful amounts, the team would first need to grow more virus particles & this can only be done in living cells – a step that was specifically excluded in the OIA request. I’ve underlined the relevant part in the screenshot below.
Let’s continue.
On the 8:24 timestamp there’s a quote from Prof Racaniello’s video lecture that is taken out of context. “…most of the time we take this nasopharyngeal swab in the solution, we just do the genome sequence and we don’t actually have a physical isolate virus and that’s very important.” According to Bailey, the genomic data by themselves do “not equate to proof of a virus.” To support this she moves to a blog post by Racaniello, which she claims shows him admitting that very same thing.
Again, as is the case throughout this video, there’s no link or url visible, but the blog post is easy to find. What the professor said was that the presence of Zika virus RNA in mice, up to 60 days post-infection, was not the same as the presence of infectious virus. She kind of left that italicised word out. In that blog post it’s clear that the virus was present in the mice at some point – because the researchers infected them with it, & so at the very least the test was detecting prior infection. (CT values on a PCR test do allow an estimation of whether someone is likely to be infectious or not.)
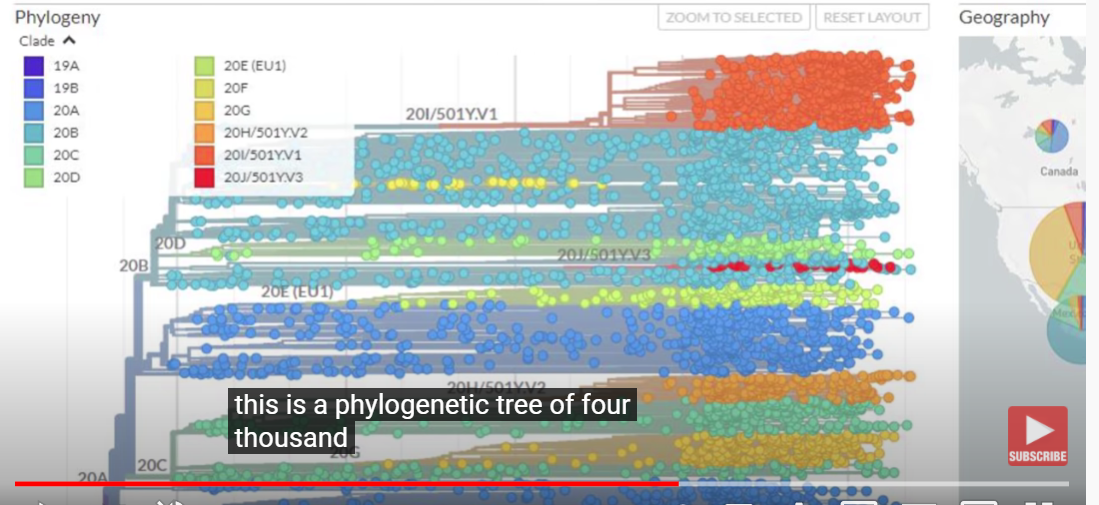
Subsequently there’s a screenshot of a Nextstrain image showing the phylogenetic relationship of SARS-Cov-2 obtained from almost 4,000 individuals (it’s a screenshot from one of Racaniello’s teaching videos, but my link is to the original on the Nextstrain site) and claims that because there were no purified samples then the whole thing is based solely on PCR tests & is nonsense. What she’s conveniently omitting here is the fact that Nextstrain’s analyses are based data from on sequencing of the entire viral genome from each of those individuals – the same sort of thing that’s done here when our Ministry of Health covid-19 team is trying to track potential chains of transmission. Racaniello’s own video describes how the information in that family tree is generated and interpreted by researchers.
However, Bailey would like us to believe that there’s no evidence that any of those genome sequences come from the virus. (Mind-boggling, I know.) As ‘evidence’ for this, she shows a screenshot from a religous organisation’s page that highlights an offer of a 1-million-euro prize to anyone who provides “irrefutable evidence” of isolation of the virus and asking why no scientists have claimed it. Again, no link – but a little detective work shows that it’s an “offer” made by a far-right German antivaccine activist. The offer has strings attached – he wants scientists to follow those original Koch’s Postulates. Hardly surprising that no serious scientist would take the offer seriously, Sam.
Next we see a screenshot from a 1978 letter to the editor of The Lancet, – again, no url or publication details. Why is that? In any case, the authors of the paper comment quite clearly (& you can see this in her screenshot) that the presence of an organism can be identified even in the absence of an isolate, by using other techniques. The image really doesn’t support the laboured point she’s trying to make.
And then, at 11 minutes 58 seconds in, we get the startling statement that the image below, which clearly shows coronavirus particles (you can see their ‘crown’ of spike proteins in the image) outside a cell is actually ‘nanoparticles’ close to a ‘cell wall’. (NB in the absence of any identification of the image source in Bailey’s video, I found it impossible to track down the original. Even Google Lens was no help.) That’s closely followed by an attempt to conflate these particles with structures called exosomes, or extra-cellular vesicles (& again we have this hang-up on definitions rather than actual science), using a screenshot from this journal article that is talking about nomenclature in a rather abstruse way, and not about viruses at all.

And then there’s “this gem of a publication that appeared in the Lancet last year” – you’ll find it here. Interestingly it includes images that the authors clearly view as SARS-Cov-2 virus particles that are near-identical to those that she characterised as non-viral ‘nanoparticles’ just a few minutes earlier in her video. Furthermore, there’s no evidence that the authors characterised other, inaccurate images as the “fraud” that Bailey claims; they say only that these latter images are too ambiguous or show intracellular structures.
In other words, the video is full of inaccuracies, misrepresentation, contradictions, and missing links.
And, verily it is said that the time & effort required to review these things far exceeds the time taken for someone else to produce them.
A Dr Bailey is a Christchurch-based GP. On her YT channel she describes herself as a “research physician” who “researches and covers common medical conditions”. Looking material up in databases or more general online sources doesn’t by itself make you a researcher; at least, not in the sense that people engaged in actual scientific/medical research programs would understand the term.
B I was also advised to buy her book (which is clearly visible in the background throughout this particular video). I did not. It’s interesting how so many of the “experts” held up by those opposed to vaccines are so keen to have you buy products of theirs. Can I say “grifters”? Yes, I can.
C Make that, rather a lot of shade: “the supposed SARS-Cov-2 tests are supposed to react to mRNA that’s specific to the virus.” That is exactly what they do; Bailey needs a refresher on how PCR operates – it’s a highly specific technology.
D This is a bit rich coming from someone who isn’t a virologist or a scientist, but oh well.
E There is more than a little hubris here, & almost a nod to denial of germ theory.
F And a nod to the conspiracy theory that the virus doesn’t exist? (see also E.)
G The results, she says, are published in her book, so we aren’t talking peer-reviewed material here.
NB: comments on this post are now closed. Partly they were becoming repetitive, but also I can do without the threats.
Howard Vickridge says:
Thanks you so much for your endless work knocking back the scientifically illiterate numbskulls. These people who shoot arrows outside their field of expertise are a real blight on wisdom, and unfortunately journalists buy their crap stories under the illusion that a ‘Dr’ of any kind is a genius of everything. GP is a specialist for sure, but is far from being a biologist, virologist, or a public health expert. That Bailey is flogging a book tells all we need to know of their motivation to shit-stir. Shame on them.
Alison says:
Thanks, Howard.
greg goodley says:
As this seems to be where the experts share their wisdom, I have a couple of simple requests, and, I am without agenda, simply seeking clear factual answers, so if you could please clarify a couple of things if not to much trouble
.1, is it possible that altered DNA and vaccines that identify a partial virus, could eventually risk a breakdown in the ability to naturally build immunity on any level, to some future flu/ virus perhaps, I’ve looked at some government studies on radio frequencies and possible links to genetic damage, and with some bad press out there with this 5g and its concentrated wave length coinciding with this somewhat testing deprived vaccine getting fired out, can anyone guarantee we are not going to be reliant on a medical companies vaccines, %?
Alison says:
is it possible that altered DNA and vaccines – I’m not sure what you’re asking here. The Pfizer & Moderna vaccines are mRNA vaccines, and neither of them can affect your DNA (they don’t enter the nucleus). Your immune system reacts to any antigen that it recognises, whether that’s presented via one of these vaccines or in the normal run of events – vaccination doesn’t “weaken” your immune system.
5G refers to “5th generation” technology; it’s at a slightly different wavelength than the current 4G but couldn’t be described as “concentrated”.
And if you’ve followed this blog, or (for example) Helen Petousis-Harris over on Sciblogs, you’ll be aware that the Pfizer vaccine has received the same rigorous testing as any other vaccine on the market.
Barry Shaw says:
Hi Alison,
So, if the Pfizer vaccine has been so rigorously tested, how come testing won’t be fully completed until 2013?
Medsafe’s conditions for it’s provisional use was only for a limited number of patients, i.e. not for general use, under the Medicines Act 23.1.
The general release by the government was challenged in the High Court on the 15th of May 2021 in Wellington, by eminent lawyer Sue Grey, for breach of the Medicines Act.
The government was found to have acted illegally.
In response the government changed the law overnight, disregarding the potential dangers to the general public of the experimental vaccine.
Alison says:
If you read the actual RCT documents and the NEJM paper describing the Phase III results, you’ll see that what continues until 2023 (not 2013) is the phase IV observation of participants, to determine how long the vaccine’s protection lasts. Phase III determined efficacy & effectiveness, information that was required for any application for approval.
As I’m sure you know, the judge in that case largely rejected Sue Grey’s claims. The judge recommended that the Government consider a law change (which subsequently happened), but declined to halt the vaccine rollout. In doing so they noted the public health importance of the vaccination program going ahead.
Enough with the “experimental vaccine” claims. It’s not.
Paul Villforth says:
Unfortunately, it seems you have missed some very important points regarding viral isolation from the surrounding soup in which the supposed virus is grown. If you read the literature you would find that the virus genome was not that of SARS-CoV-2 but was composed of pieces from a genome library of SARS-1.
The CDC was asked through Freedom of Information Act requests if the CDC knew if they had any SARS-CoV-2 isolated virus or purified samples of the virus. The CDC’s response was that they did not know of any SARS-CoV-2 virus purified material anywhere in the world.
What is also not known until the CDC was tasked with additional FOIA request regarding viral isolation of previous virus vaccine manufacturing and the answer was that no virus in the past 70 years has ever been isolated and or purified. When I read that I was very surprised, because virologists that have taught courses I attended in the 1970s always claimed that vaccines were based upon purified strains of viruses.
The supposed method of isolation and purification also include a step that has been ignored this time around. The supposed viral isolate or purified virus is tested on animals to see if they got it correct. That is the only way to know for sure that what you have is the actual virus. No animal studies have been done with the supposed isolated virus not have any animals been used to test the non-vaccine vaccines. Humans are the test animals this time.
The CDC used to have a paper describing the isolation but it has been taken down when they were told that it was a case of fraud since no isolation of any kind was done. There are ways to tag the protein coats of viruses so they cane be identified when they are in a soup of other materials. This has yet to be done. Then there are the autopsy results for the UK and Europe that showed that people were dying from a bacterial infection, not SARS-CoV-2.
Then there is a recent announcement from Canada that the Pfizer and Moderna vaccines are creating the virus in those vaccinated. The claim is that the vaccine designers didn’t know that the spike protein is the actual cause of the disease and can be discharged from the vaccinated person’s lungs. The vaccinated have become spreaders of the disease that is now a manufactured virus with a synthetic spike protein that doesn’t behave as the original. Some are calling it a bioweapon.
Alison says:
The CDC was asked through Freedom of Information Act requests if the CDC knew if they had any SARS-CoV-2 isolated virus or purified samples of the virus. The CDC’s response was that they did not know of any SARS-CoV-2 virus purified material anywhere in the world. This might have been true early in the pandemic. It’s certainly not the case now, & hasn’t been for quite some time: https://www.cdc.gov/coronavirus/2019-ncov/lab/grows-virus-cell-culture.html
CDC was tasked with additional FOIA request regarding viral isolation of previous virus vaccine manufacturing and the answer was that no virus in the past 70 years has ever been isolated and or purified. And I’ll call BS on that one: https://www.cdc.gov/vaccines/pubs/surv-manual/appx/appendix07-meas-vi.pdf
How exactly do you think live- or attenuated-virus vaccines are manufactured?
The supposed viral isolate or purified virus is tested on animals to see if they got it correct. – since many viruses are host-specific, that is not going to be much use, is it?
Alison says:
The CDC was asked through Freedom of Information Act requests if the CDC knew if they had any SARS-CoV-2 isolated virus or purified samples of the virus.
I strongly suspect that the FIA requests were worded in an identical way to that used by antivaxxers in NZ: a way that excluded viruses grown in cell culture. Since viruses can only be grown in cell culture, it’s hardly surprising that the answer was in the negative.
Alison says:
No animal studies have been done with the supposed isolated virus not have any animals been used to test the non-vaccine vaccines. Also BS, as the Pfizer vaccine was tested in macaques & mice: https://www.reuters.com/article/factcheck-covid-vaccine-animal-idUSL2N2NJ1IK and https://www.nature.com/articles/s41586-021-03275-y
the autopsy results for the UK and Europe that showed that people were dying from a bacterial infection, not SARS-CoV-2. – citation please.
that the Pfizer and Moderna vaccines are creating the virus in those vaccinated. – and that is an utter impossibility.
Kathleen M says:
‘Then there is a recent announcement from Canada that the Pfizer and Moderna vaccines are creating the virus in those vaccinated.’
I’m a healthcare provider in Canada, we ‘announced’ no such thing.
Paul Villforth says:
The mRNA vaccine components can be incorporated into your DNA through reverse transcriptase. This is available in the cell cytoplasm as well as in the nucleus. It is used to repair DNA and the mRNA vaccine could be accidentally or deliberately included in your DNA using reverse transcriptase. In fact, this is how DNA is changed to improve the species over time.
It was originally thought that the shot would stay in the muscle or remain close to the injection site. We now know from reports from Canada that the spike proteins are in major organs within 10 hours of the injection. In females the spike proteins are seeming to proliferate in the ovaries. They are also being found in the liver, bone marrow and spleen. We are seeing clotting disorders because that is one of the things the original spike protein did and it seems the synthetic spike is capable of the same thing. The original disease also caused miscarriages so why are we now injecting pregnant women with a vaccine that has the disease agent? Seems to be a case of stupidity. The vaccine manufacturers may have limited liability protect in the US but they don’t have that anywhere else in the world. There are the beginnings of lawsuits in European countries against the vaccine manufacturers.
If the vaccines have been rigorously tested as you claim why hasn’t the data been released?
Alison says:
The mRNA vaccine components can be incorporated into your DNA through reverse transcriptase. It might be if we had reverse transcriptase in our cells. We don’t. What we do have is a polymerase that may be involved in repairing errors in DNA, using our own transcribed mRNA as the template to do that. (Since there’s no DNA sequence that is a close match for the spike protein mRNA, the mechanism you propose seems unlikely.)
In fact, this is how DNA is changed to improve the species over time. – just, no. Species don’t “improve” over time; they become better adapted to current circumstances. While retroviruses – which do possess reverse transcriptase enzymes – can insert themselves into our genome, they may or may not have had an evolutionary impact on us. Most of the genetic variation needed for evolutionary change arises through mutations.
from reports from Canada – citations please.
In females the spike proteins are seeming to proliferate in the ovaries. – citation definitely required. The only paper suggesting this uses a rat model.
it seems the synthetic spike is capable of the same thing – since the vaccine spike protein is locked in a conformation in which it cannot interact with cell membrane receptors, citation please.
with a vaccine that has the disease agent – it doesn’t. The “disease agent” is SARS-Cov-2, not the S protein.
but they don’t have that anywhere else in the world https://www.stuff.co.nz/national/health/coronavirus/300213490/government-grants-vaccine-suppliers-indemnity-against-claims
If the vaccines have been rigorously tested as you claim why hasn’t the data been released? oh, come on! Really? The Phase III results were publicly available at the time the FDA gave emergency use approval for use in the US. https://www.fda.gov/media/144245/download They were also presented by publication in the NEJM. https://www.nejm.org/doi/full/10.1056/nejmoa2034577
Steve says:
Vincent Racaniello interviewed Fauci, and Fauci confirmed that with PCR testing above 35, the odds of determining an accurate test result are “miniscule”. Indicating completely unreliable testing levels.
Watch here at 40 seconds:
https://www.youtube.com/watch?v=A867t1JbIrs
So why are people testing about 35x all the up to, and over 40x, and claiming the test results are accurate?
Something extremely disturbing is going on here with this pandemic. It is not passing the smell test.
Alison says:
Why not link to the actual This Week in Virology recording? Could it be that the YT video has been cherrypicked? (I suspect so since the original interview by Dr Racaniello on TWIV is considerably longer than 40 seconds.)
What Dr Fauci actually said was that with samples that give a positive result only at high CT values, the odds that the person is infectious are miniscule & the results are generally interpreted as meaning the patient is not contagious (what we’d call an historical case in NZ).
For those interested, there’s a summary of the interview/discussion here & the inteview itself (from July 2020) is available on the TWIV podcast page via i-tunes.
Debbie says:
So you think any virologist, gp, medical practitioner, researcher etc is only worth listening to as long as they hold the same opinion as you or the mainstream narrative? How very biased of you and you should be ashamed of yourself!
Alison says:
No, I expect them to provide accurate, evidence-based information, a criterion that Dr Bailey repeatedly fails to meet.
Darren says:
Sorry Debbie but Alison is performing a valuable service here. And she isn’t dispensing opinion but facts with references. You and I would dispense opinions because we’re uneducated in this field of expertise. Unfortunately it appears this is also the case with Sam Bailey. She’s not even vaguely trained in the fields of virology or epidemiology (as best I can tell her speciality is as a surgeon https://www.mcnz.org.nz/registration/register-of-doctors/doctor/bailey-samantha-annabel-hope/) but is portraying herself as an expert in those fields and saying some things which are just flat out holy cow stupid. And it does seem to be to sell a book.
She’s likely never seen a patient with COVID let alone treated one but despite this lack of education, training, or hands on experience is dispensing advice from an assumed position of authority which could potentially lead to many deaths.
Thanks again Alison. Keep it up.
Alison says:
Thanks, Darren, I certainly will!
Dallas Knight says:
Yes, thank you for this pushback. Dr Sam Bailey is gathering many followers with her messages of misinformation YouTube and Odysee. These messages need to be addressed in detail such as you have done.
Alison says:
Thank you for the positive feedback 🙂
Kate says:
I cant see how to start a new comment so putting this in a ‘reply.’ Im still sifting through Dr Sam Bailey’s material but in terms of her expertise, mentioned above, her main job included 10 years in clinical research – so she is both a scientist and a researcher
Alison says:
Her “main job” was as a GP. She was associated as a practitioner with a cardiac research group at Otago University ie she was part of a research team. However, she has no training as a scientist & so it’s a stretch to call her one. A “research practitioner” would be a better term.
Smut Clyde says:
it’s an “offer” made by a far-right German antivaccine activist.
Eckert started out as a televangelist but he shifted to antivax scamming as even more lucrative.
Alison says:
Yes, I noticed that when I was tracking down her image source.
David says:
Thanks for your hard work here!
There are far too few people countering this person. I tried raising a few of the points about her claims it being a mess and that the virus hasn’t been isolated. Also her seeming confusion over isolates isolate and purification on the video in question and I’m certainly no virologist!
Alison says:
Hey, thank you! I might summon the intestinal fortitude to look at another of her videos 🙂
Michael Dawson says:
Why don’t you contact her and debate her?
Alison says:
Because science doesn’t work by debate of the sort you’re suggesting.
Matt Tucker says:
Hi Alison,
thanks for you assessment. I think you miss the point of Dr Bailey’s video regarding the fact that people are talking about different things when they say “isolation” of viruses. As she points out Vincent Racaniello also admits this – the language has confused both scientists and the public. I think your article is weakened by questioning Bailey’s motives and the authenticity of the references which are usually all cited with all her videos. (Not sure if you realised the references are in the video description?)
I don’t think she works as a GP anymore, she states in a video about clinical trials that she is a research physician in later stage clinical trials (https://www.youtube.com/watch?v=7h7mLhjYvF8).
One point you miss is the uncertainly of the provenance of the nucleic acid sequences. Dr Bailey is certainly not the first to raise this question. The sequences are put together from cell cultures which contain millions of bits of nucleic acids, how do we know they come from inside a virus?
Did you try to contact Dr Bailey? I’ve emailed her previously and she responded quickly to some questions I wanted clarified. She is very friendly and you might even learn something new!
Alison says:
“how do we know they came from inside a virus?” – because the virus has actually been purified, Dr Bailey’s claims notwithstanding. I’ve even provided links to papers explaining how that’s done; perhaps you didn’t read those? So no, I haven’t missed that point.
Not sure if you realised the references are in the video description? – I certainly didn’t see them. As to motives, they seem fairly obvious. Starting with “buy my book”.
Alison says:
And see also this thread, written by an actual virologist.
https://www.reddit.com/r/medicine/comments/g8mjmo/has_a_patientfamily_memberfriend_told_you_that/
Karlene Guthrie says:
Very well written and cited. I learned a great deal. Thank you.
Jason says:
The idea of whether or not the virus has been isolated or purified is rather pointless. Dr. Bailey nor the offer to anyone who can isolate the virus mention Koch’s postulates.
One of the papers that is linked in this piece, purporting to have isolated the virus states, “These findings strongly urge the need for comprehensive studies that combine genomic data with epidemiological data and clinical records of symptoms from patients with COVID-19” If you read the paper, you will see that the genomic, epidemiological data, and clinical presentations have not all been linked together by this “isolation.”
Dr. Mullis, the inventor of PCR never claimed it to be diagnostic tool, and, in fact, he claimed that the HIV virus was not the cause of the illness AIDS. I know a lot of people who had “positive” tests but never got sick. And nobody around them got sick.
Alison says:
I’m not sure why you feel it “pointless”, given the frequent antivax claim that isolation & purification haven’t happened. Certainly Dr Bailey’s video is fairly pointless, since she’s arguing semantics rather than science. And of course those doing the isolation don’t mention Koch’s postulates, because they’re aware that those original postulates do not & cannot apply to viruses.
Clinical presentations are of the disease, covid-19; the genomic work shows the presence of the virus itself, SARS-Cov-2.
And you’re wrong that Mullis never claimed that PCR could be a diagnostic tool. The statement that it could be used that way is included in the original patent. He backpedalled on that when he shifted to HIV/AIDS denialism. Your personal anecdote proves nothing at all.
Jason says:
That’s exactly why– I feel that it is pointless to debate with anti vaccine people, which is certainly different than discussing the pros and cons/risks and benefits of vaccination with someone who doesn’t have outrageous beliefs that vaccines are going to be used for tracking the population, or to sterilize people, and so forth.
Koch’s postulates are outdated; as you pointed out, Koch himself changed his mind when he found that there can be asymptomatic carriers. However, you mentioned Koch’s postulates whereas, Dr. Bailey and the group offering the prize did not.
The video by Dr. Bailey does indeed argue semantics. But it’s worth mentioning that semantics have been used to manipulate the public during the corona virus pandemic. WHO changed its description of herd immunity to say that herd immunity comes from vaccination. Yes, it can come from vaccination, but also from those who recover from the illness and develop antibodies. Every pandemic in history ended without a vaccine. The concept of herd immunity was also misrepresented as “No Covid, at all.” In fact, herd immunity means that it could still exist as an endemic illness.
I haven’t read the original patent for PCR, but as a diagnostic, it has been unreliable. Not too long ago, PCR diagnosed a false whooping cough epidemic here in the US;
https://www.nytimes.com/2007/01/22/health/22whoop.html Who knows how many Covid cases were false positives? Here in the US, the governor of the state of Ohio had a positive test, and he didn’t want to isolate, so later the same day, he got a negative test. Elon Musk had both positive and negative tests. Many of the US pro football players had to miss games because they tested positive, but most of them never got sick at all.
Alison says:
Bailey didn’t reference the postulates by name, but she was certainly doing so implicitly, in repeatedly referring to bacterial isolation standards. Similarly, since those offering the prize also reserve the right to make the decision, I’m certain they would have pulled the KP card if anyone applied for the prize. We’ve seen how these things play out already (https://en.wikipedia.org/wiki/David_Bardens)
Yes, WHO changed its definition – to reflect the fact that it favours achieving community immunity via vaccination rather than by mass infection. Ethically that’s an improvement, given the relative risks of the two approaches.
False positives exist with any test. For PCR, the papers I’ve read put the incidence of false positives at less than 10%. Regarding the NYT story you link to: “With pertussis, she said, “there are probably 100 different P.C.R. protocols and methods being used throughout the country,” and it is unclear how often any of them are accurate.” Where a single, standardised test is being used (& used correctly) then this is much less of a problem. Remember that the technology has moved on in the last 14 years.
“Many of the US pro football players had to miss games because they tested positive, but most of them never got sick at all.” – it’s not only about getting sick, though, is it? It’s also about reducing transmission to others.
Geir Holst says:
It is all about health, and that is not getting sick or ill or depressed or deprived.
That’s hard to understand from a position of privilege to protect 🙂
And then the medication should not be more pricey then the sickness.
Alison says:
The vaccine’s free in NZ, Geir.
Ginny says:
If the virus was isolated then why couldn’t there be a standard vaccine based on the virus created, rather than the experimental and highly controversial MRNA one?
I think because of your clear “I want to attack this person, because their opinion isn’t in line with governmental bodies” approach in this article undermines most of what you are saying.
She is very straight forward, open and prepared to debate. Unlike most of the crowd out there. Very interesting videos on government responses to one microbiologist (NZ) letters. Why don’t you write an article on that?
Attack the argument, not the person, then maybe you can be taken seriously.
Alison says:
You seem to be assuming that I work for a “government body”. I don’t.
mRNA vaccines are much faster to make than “standard” ones, because there’s no need to grow up very large amounts of actual virus particles. They also contain far fewer ingredients, which I would have thought those opposed to vaccination on the grounds of all those ingredients would view as a plus.
Very interesting videos on government responses to one microbiologist (NZ) letters. Why don’t you write an article on that? Partly because I have no idea what you are talking about. And partly because I write on subjects that I choose. Since blogs are easy to set up, if this is a topic that interests you, you could perhaps write your own blog about it.
Attack the argument, not the person, – you seem to have missed the fact that I did.
shina says:
well said
Ginny says:
The whole ‘it’s about reducing transmission to others’ argument is getting so lame. Nobody in the world cared about that regarding seasonal flu (kills all ages), STDs, or other heinous diseases like swine flu and meningitis. What about respiratory disease, our third biggest killer? Killing more Kiwis every year than the old wuhan flu.
Give us a break, most people are sick to despair of the hype and spin around corona, sorry wuhan flu, sorry covid-19, sorry bat flu, sorry world control flu. More chance of getting hit by a car walking in a clown suit, juggling a ball and eating a cherry ice cream, than ever having to worry about dying of this virus.
Dr Sam is a breathe of fresh air in these insanely perverse, corrupt and undemocratic, lack of debate and discussion, oppressive times.
Alison says:
The whole ‘it’s about reducing transmission to others’ argument is getting so lame. Nobody in the world cared about that regarding seasonal flu (kills all ages), STDs, or other heinous diseases like swine flu and meningitis.
Let me see: we have vaccines against seasonal flu, meningitis, and at least some STDs (hepatitis B & HPV). A vaccine was also developed against the H1N1 swine flu in 2009. So it’s completely incorrect that “no-one in the world” cared/cares about reducing transmission of these infections.
What about respiratory disease, our third biggest killer? Killing more Kiwis every year than the old wuhan flu.
Which “respiratory disease” would that be? Here’s a ranked list of the leading causes of death in NZ, 2010-2012: https://www.health.govt.nz/our-work/populations/maori-health/tatau-kahukura-maori-health-statistics/nga-mana-hauora-tutohu-health-status-indicators/major-causes-death
Similarly the Insurance Council of NZ identified the top 3 causes of death in NZ in 2015 as cancer, heart attacks, and strokes:https://www.lifecovered.nz/life-insurance/leading-causes-of-death-in-new-zealand/
Your vague “respiratory disease” doesn’t figure in either.
Give us a break, most people are sick to despair of the hype and spin around corona, sorry wuhan flu, sorry covid-19, sorry bat flu, sorry world control flu. More chance of getting hit by a car walking in a clown suit, juggling a ball and eating a cherry ice cream, than ever having to worry about dying of this virus.
I’m sure the families of the 3.3 million globally known to have died from this virus (so far) would beg to differ with you. The odds of dying of it here in NZ are currently very low; you might like to reflect on why that is.
As for the rest of your comment – I hadn’t noticed debate or discussion being “stifled”. If that was the case you would not be able to comment here.
Bolly says:
Well said and as for cases asymptomatic cases. That could simply mean no wuhan variety just something of mRNA that triggered a positve response with a PCR test and it is recorded as covid [Wuhan style] positive.
Absolute inaccurate statistical B/S
Alison says:
“Asymptomatic” means “infected but not showing any symptoms. PCR testing is accurate enough to be able to tell if it was a covid19 (SARS-Cov-2) infection or not.
Lazlo says:
Ginny, people need their funding so they have to fit in with the narrative otherwise they won’t be able to do their research.
Therefore enlightening debate on these types of blogs is futile
I could recommend a few others worth reading
Alison says:
I wouldn’t say that Ginny was providing “enlightened debate.”
And I’m not paid to blog, so your $hill gambit is null & void.
shina says:
exactly
arthur brogard says:
Very interesting but also very confusing in the end.
Needs some clarification I think. Or I’d like some.
I don’t care much about the fine detail or the personalities.
Just: What was Dr Sam trying to say?
Was she right or wrong?
And by that I mean the ‘main thrust’ of her video.
Alison says:
Dr Bailey was trying to say that the SARS-Cov-2 virus has never been isolated. She was & is wrong.
Lazlo says:
She’s not wrong
Alison says:
In your case, that which is asserted without evidence can be dismissed without evidence.
sagymrat says:
Interesting comment, please contact her and arrange a discussion to clarify her perspective vs yours..
Alison says:
And give her another platform? I don’t think so. Her perspective is quite clear, & so is mine: she’s made multiple claims about covid-19 that are not supported by actual science, & which seem to contain a fair amount of misinformation & misdirection.
Deborah says:
And unlike Sam Bailey you don’t have a “buy me coffee” or buy my book plea right under her video.
Thank you for your time putting real research ahead of muppet madness. I think most of them are still waiting for the Oprah style free car on Sam’s channel ????
Nothing like a charismatic good looking person who claims they are an expect to mobilise the muppets.
Lana says:
Thank you for your work!
Here’s the paper Bailey uses (but does not cite) to make up stories about exosomes. The CoV2 isolates and methods are all described by the authors and the images are literally cutting edge.
https://www.nature.com/articles/s41598-021-82852-7
Enjoy!
Alison says:
Thank you! I’m staggered that she’d use a paper describing the virus & its isolation to claim it hasnt been isolated.
sb says:
a) The methodology, in summary, describes mixing “virus stock” with Vero E6 cells, incubating and fixing, and then centrifuging. It was then prepped for sectioning and then electron microscopy. This does not mean they had a purified sample of “SARS-CoV-2”.
b) The EM photos are claimed to show the virus particles but how is it possible to distinguish these from extracellular vesicles? Basically it is not possible.
c) Figure 5 shows the scatterplots with maximum diameter of the “virus” particles on the x-axis. Note how it ranges from around 85-155nm – rather large variation for a supposedly simple entity such as a virus.
Alison says:
a) it certainly does mean they had a purified sample – ultracentrifuging is routinely used to separate out cell contents, & has been for years.
b) it’s called a coronavirus for a reason. Extracellular vesicles dont have a corona of spikes. And as another commenter has pointed out, the image Dr Bailey claims to show vesicles is from a Nature paper describing isolation of the virus.
c) why equate size & “simplicity”? And no, in nm this is not really a large range. The mean is the important value.
SB says:
a) ok, your right: ultracentrifuging is the method to separate super tiny things from each other. but it has its limitations and it is just one step in the identification process. you need to use an another method to identify the entity you are looking for. and there is the challenge in the further investigation. you say it is easy: ultracentrifuging + take a photo = you will have the perfect result. but it is more complicated with a lot of possible error.
b) it seems to me that it is not that clear. Dr SB is right when she says, it is not so obvious what we can see under the EM.
ECV: https://www.cell.com/structure/fulltext/S0969-2126(14)00294-9?_returnURL=https%3A%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0969212614002949%3Fshowall%3Dtrue
It seems to me also that flu virus has also a very similar shape and structure under the EM: https://www.pnas.org/content/103/50/19123
c) there is no equivalence between size and simplicity in my message. it is a simple fact: there is a large variation between the sizes. is it not true?
“the mean is the important value” from which perspective? it is true when you believe that you see your wanted viron on that picture.
Alison says:
a) Well of course they use other methods to “identify the entity” – PCR testing (which is highly specific) springs to mind.
b) Notwithstanding your “it seems to me” statements, what’s visible in those EM images was clearly identified as coronavirus by those who wrote this particular paper (and those who wrote multiple others on the same lines). Dr Bailey is not exactly an expert in this field.
Influenza isn’t a coronavirus.
c) – not particularly. The dimensions allow them to determine if particles are likely to be virions; afaik it’s not a diagnostic for any one particular virus.
Barry Shaw says:
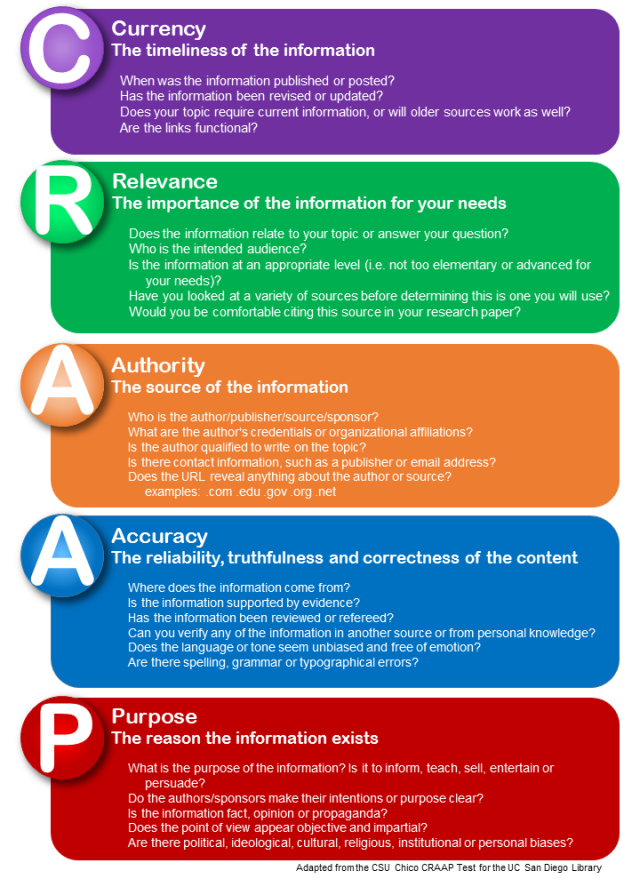
Am I missing something … the heading of this bioblog is CRAAP?
Alison says:
haha, very droll. The featured image at the top of this particular post shows the CRAAP detector, a tool that’s increasingly used in schools and universities to help students assess the validity of materials & resources they come across. Sam Bailey’s post does poorly against it.
Paul, says:
Asymptomatic spread ?,after 18 months of this pandemic I have been aware of three cases from associates of confirmed covid cases , two of them were spread from people with mild symptoms ,both among friends,,the third person, son to father,(that became very sick)though it’s not known if the son was showing symptoms in this second hand info,it’s rumoured the first two mentioned cases are that the young men had been sharing their smokes which would be very high risk behaviour,Seems to me asymptomatic spread is nearly false.
Alison says:
Unfortunately personal experiences are at the level of anecdote. Large-scale analyses show that asymptomatic spread is reasonably common: https://www.thelancet.com/journals/lanepe/article/PIIS2666-7762(21)00059-4/fulltext
sb says:
this whole comments section is very problematic. slow & cumbersome. and the conversation is also very superficial and biased, mostly. all arguments are very soft, so both sides can argue pro and con at will. it’s all about you being biased in a different way than those who write, trying to write some pithy response to everything to make it seem like you’re right. it’s all a crock.
Alison says:
You’d prefer I didn’t reply? Since quite a few of the commenters on this particular post appear to be apologists for Dr Bailey, that is unlikely to happen.
The comments section is set up (by the Uni IT folk) in the way it is because about 99.9% of “comments” are either spammers or scammers, most of whom are pushing some version of erectile disfunction pills. Even with filters quite a bit still comes through to me. Hence the wait for comments to be approved, as I’m not constantly checking the page.
Scott says:
Thank you Alison…..your responses have been very much to the point
Maren says:
I find myself never knowing which side to take over the last year. It’s obvious though, that there is a lack of logic when it comes to how we must protect ourselves from COVID. I know many people who have had COVID and suffered much like one does with the flu. I have always questioned the flu vaccine, after having been vaccinated and then falling sick from it.
Is the future a life of yearly vaccines for “hopeful” protection? Do I vaccinate my children against Covid-19 and if so, at what cost to their future health? If children are not vaccinated but can carry the sickness then how is herd immunity achieved?
I want logic in a world that has been made completely illogical seemingly due to a flu bug type sickness!
Alison says:
No vaccine offers 100% protection from a pathogen.
there is a lack of logic when it comes to how we must protect ourselves from COVID. – not sure what you mean by “a lack of logic”. Taking steps that reduce transmission of an airborne pathogen (masking, physical distancing, good “cough/sneeze hygiene”), plus use of vaccines with high efficacy, are logical steps to take in this instance.
You’re right, we probably won’t achieve community immunity until the majority of children have been vaccinated. This is a significant problem in dealing with this virus.
a flu bug type sickness – it most definitely is not. In a “bad” flu year, the flu kills around 60,000 people in the US. Covid-19 mortality there is at least one order of magnitude greater, & that’s not including the impacts of “long covid”.
Maren Briggs says:
Will we soon be vaccinated for every virus that appears?
There is a 99.97% survival rate for Covid for those under age 50. The death toll counts have admittedly been incorrect with the USA counting many cases who weren’t solely caused by Covid. Now the data is in that those under 20 should not be vaccinated.
Why all this for something not as deadly as we were made to think? I don’t see the logic if there will always be new variants that the vaccine may not protect against. It’s frightening when something is so magnified by politicians and the media. I worry whenever people just fall into line without question.
Alison says:
Will we soon be vaccinated for every virus that appears? – I doubt it: only for the ones that cause significant morbidity & mortality. (There are millions of different viruses and most of them are quite innocuous from our perspective.)
There is a 99.97% survival rate for Covid for those under age 50. Firstly, the figures aren’t so good for the over 50 demographics, are they? And secondly, the law of large numbers means that in a group of 100,000 under-50s you’re still seeing 3,000 deaths. You’re OK with that?
Now the data is in that those under 20 should not be vaccinated. – citation required for that one!
Why all this for something not as deadly as we were made to think? – 600,000 deaths in the US. 500,000 in Brazil. 400,000 in India (& that is probably a significant underestimate). Nearly 4 million deaths globally. I’d hate to see how many deaths you’d accept as “deadly”.
Maren Briggs says:
Of the COVID-19 deaths reported, many were associated with pre-existing conditions and many were incorrectly reported. I have associates in the medical and emergency industry who were infuriated at having to mark the cause of death as Covid when it really was not. For example a motorcycle accident and the man is bleeding out and tests positive for Covid19, guess what the reason for death was?!
The WHO just put this out in regards to vaccinating those under 18. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice
Life after 50 is precious. More than 50% of Covid deaths occurred in those aged 80 and over. We have pushed life expectancy back and now to save those who are 80,90+, we restrict the lives of those who are 20,30+. At age 80 one has a 12% risk of death from Covid19.
I am still looking for logic, when we have forgotten all the other potential risks for death. What about all the harm that mask wearing, confinement, and fear is causing for the young. What will their future mental health look like?! I can’t help but think there is something more going on here.
Alison says:
many were associated with pre-existing conditions – this doesn’t mean that they were going to die of those pre-existing conditions, does it? People with high blood pressure, diabetes etc can manage these conditions successfully & make meaningful contributions to society (not only economic contributions) for many years. And in very many cases were doing that right up to the point where they contracted covid-19.
In addition the risks of increased hospitalisation & death increase well before you hit your 50s: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html
You should also read this: https://www.nature.com/articles/s41591-021-01437-z
Luke says:
Won’t the virus just mutate again and again even with the vaccines? And also with the synthetic spike proteins won’t our bodies depend on consent vaccines? And sorry one more thing have you seen Covax 19 isn’t that a better method?
Alison says:
Won’t the virus just mutate again and again even with the vaccines? – yes, but with a large enough population vaccinated the rate should effectively slow. That’s because if the virus gets fewer chances to replicate (lower viral load &/or shorter infection duration) then it also has fewer chances to mutate.
And also with the synthetic spike proteins won’t our bodies depend on consent vaccines? – no more than for something like the flu, which mutates regularly. (Not sure what you mean by “consent vaccines” since all vaccines require consent from the vaccinee.)
And sorry one more thing have you seen Covax 19 isn’t that a better method?
No-one can make that call as Covax19 is in phase II trials at the moment. I’m not even sure that the Phase I results have been published, tbh.
Brian Sandle says:
Alison wrote: “You’re right, we probably won’t achieve community immunity until the majority of children have been vaccinated. This is a significant problem in dealing with this virus.”
Though I understood the vaccine does not stop a person being infected. It helps them have fewer severe symptoms and by that means may reduce transmission.
Besides look at antigenic competition. New strains could be at an advantage in vaccinated people?
Alison says:
If vaccination does reduce transmission, then that is a good thing. Even better is the fact that it reduces the severity of symptoms in those vaccinated.
They could be – though it doesn’t seem to be an issue with the Delta variant.
mb says:
Well, then take the jab and leave the medication for what they are. Good luck ! Who would benefit from that ?
Although, if there’s really a virus (there are hundreds of billions), it’s IFR is around 0,15 % overall. No worries for a healthy person. Otherwise most things in life would be a problem and danger.
Alison says:
Well, then take the jab and leave the medication for what they are. Good luck ! Who would benefit from that ? Might be helpful if you could express what you intended to say rather more clearly.
if there really is a virus – thank you, I have now filled today’s antivaxxer bingo card.
it’s IFR is around 0,15 % overall. No worries for a healthy person. Since SARS-Cov-2 has now killed 600,000 in the US alone, you might want to reconsider your rather callous point of view.
Johnny Dollar says:
You would be better off looking for the original author of “cov2” and and analyzing his research paper which describes how he went about crafting a sequence for cov2.
You are off the mark with this observation: “The viral genome was described – and shared globally [by https://www.sciencedaily.com/releases/2020/01/200131114748.htm%5D– a little earlier, in mid-January that year.”
The “Institut Pasteur” had nothing to do with introducing the viral genome to the world.
The Cov2 sequence was created by this man – Yong-Zen Zhang. He was the one who introduced the sequence of cov2 to the world, a sequence he stitched together using a laughably poor analysis coupled with a few lies thrown in for good measure.
Here, read about it: https://www.nature.com/articles/s41586-020-2008-3
Alison says:
The reference I provided predates the one by Zhang et al, so I’m not sure what your point is.
But I see that you find it remarkably easy to accuse people of lying from behind your pseudonym.
AJP says:
Thank you for this analysis. It highlights Dr SB’s (together with the above comments) scientific illiteracy sadly.
Just because you have access to a scientific paper doesn’t mean you can actually read and understand it. There is a reason why people spend years at university to study varies fields. It also takes years to learn to write a paper and how to read, understand and critically evaluate one. Understanding a scientific paper actually requires learning about the methodology and background, which if you don’t have scientific training you are highly likely unable to understand the content. And again that’s why scientific papers are peer reviewed by people in the same field of study who understand the intricacies and importantly the scientific concepts.
I have watched a couple of Dr SB’s videos and as a biologist I am appalled but also sadly not surprised. What can you expect from someone who has never carried out any of those techniques that she mentions, or spent any meaningful time in a lab.
shina says:
The covid19 PCR test has NO GOLD STANDARD. The binary results of positive/ negative depends on cut-off CT values which VARY from lab to lab, kit to kit. The world has been misled. NO thanks to Christian Drosten and co.
Alison says:
The CT values don’t vary in the way you imply. High CT values indicate either an historical or a very early infection, that’s all, & it’s why a 2nd test is done to confirm.
shina says:
Bayley is not wrong
Alison says:
That which is asserted without evidence can be dismissed without evidence.
sagymrat says:
BIt of a cop out statement; achieves nothing.
Appreciate your comments, but please consider contacting Dr Dr. Sam Bailey to setup a 1:1 discussion.. That would certainly help clarify things.
Michael Crowe says:
From the study on macaques
None of the challenged macaques—whether immunized or not—showed clinical signs of illness (Extended Data Fig. 7c–f). Radiographic abnormalities were generally minimal or mild, and were not consistently associated with viral challenge (Extended Data Fig. 8a, b). The histopathology of necropsy specimens obtained 7–8 days after challenge revealed localized areas of pulmonary inflammation that were limited in extent even in the control macaques challenged after mock immunization with saline (Extended Data Fig. 8c). We conclude that the 2–4-year-old male-macaque challenge model is primarily a model of SARS-CoV-2 infection rather a model than of COVID-19 diseae.
Alison says:
It’s the norm to provide a citation to accompany an extensive quotation such as yours. This appears to be the source: https://www.nature.com/articles/s41586-021-03275-y
The following quote is from the same paper:
Both candidates protected 2–4-year-old macaques from challenge with infectious SARS-CoV-2, and there was reduced detection of viral RNA in immunized macaques as compared to those that received saline. Immunization with BNT162b2 provided particularly strong RT–qPCR evidence for protection of the lower respiratory tract, as demonstrated by the absence of detectable SARS-CoV-2 RNA in serial bronchoalveolar lavage samples that were obtained starting 3 days after challenge. The lack of serological response to SARS-CoV-2 challenge in BNT162b1- or BNT162b2-immunized macaques—despite a neutralizing response to challenge in control-immunized macaques—suggests suppression of infection by the vaccine candidates. Clinical signs of disease were absent, and radiological and pathological abnormalities were generally mild after challenge. As in other published reports of immunization and SARS-CoV-2 challenge of nonhuman primates, there was no evidence of vaccine-mediated enhancement of viral replication, disease or pathology37,38. The interpretation of vaccine-mediated protection in nonhuman primates is limited by the small number of animals and the inherent limitations of animal models. Nevertheless, these preclinical results provided key support for the immunization of large numbers of clinical-trial participants with BNT162b2.
That paper also clearly negates claims that a) no animal studies were done on the Pfizer vaccine & b) (contradicting the first) that animal trials were done and all animals died as a result of the vaccine.
Michael Crowe says:
Thank you for your explanation of citation methods. I was referring to the paper named on this lengthy blog post, and I don’t believe that many other macaque studies exist. My point stands. Macaques did not die. The paper proves stuff about RNA injections inspiring monkey’s bodies to produce what researchers call antibodies. And …?
Alison says:
And so we know the vaccines did what they were intended to do. You seem determined to flaunt your inability to read the paper with understanding.
Michael Crowe says:
In Canada, excluding managed care homes, which the army blew the whistle on when they were called in to care for people who had been abandoned in squalor and filfth. in one year, less than 5,000 people died of a population of 38 million.
Alison says:
“excluding special care homes” – seems an attempt to minimise the deaths in Canada. Which, incidentally, now stand at 26,000+.
The comment about managed care homes is also an unpleasant overgeneralisation, given there were and are very well-managed elder care homes in Canada which also suffered high infection & death rates.
Michael Crowe says:
Thank you for the reply, you are certainly very fast, literally within minutes. I understand it’s unpleasant to set aside the unique population of managed care homes, but it’s also unpleasant to murder monkeys, and my point stands about how few people died in the year in question.
Michael Crowe says:
Managed care homes suffer high rates of mortality. Stop the presses.
Alison says:
You cant have it both ways. First you imply covid ravaged those homes, now you say it’s normal.
Kathleen M says:
Hey Michael. I’m a Canadian healthcare provider who provides infection control management in a non-profit Long Term Care facility. The vast majority of deaths in LTC came from for-profit facilities that cut corners, staff inadequately, and provide subpar care. That’s a huge concern. But don’t kid yourself – my facility of 200 lost over 50 residents in a year to Covid, and while our death rate was lower than the for-profits, we still experienced profound illness and loss of life.
Plenty of people in my country have died from Covid outside of care homes. We also had lockdowns, mitigation strategies in place, and the fact it targeted a vulnerable population in congregate settings surprised no one.
Michael Crowe says:
You refer to viral isolation but omit to explain the step where computers sort through genetic samples to arrive at a putative viral sequence. So what is shown is that genetic sequences can be isolated that coexist in nasal samples from around the world. Dismissing Koch’s hypothesis is dangerous because, well, Koch did. And he had to flee Germany to exile in Egypt because Tuberculin killed so many peoples’ children. https://en.m.wikipedia.org/wiki/Tuberculin
Michael Crowe says:
Similarly, Pasteur was a fraud, Rockefeller a thief and a fraud (his father a con artist and yes, purveyor of patent medicines)… the Nobel brothers who controlled the other 10% of the world’s oil were war profiteers, the Gates Foundation is a pseudo charity and media operation engaged in fake charity work designed to evade taxes while inflating pharmaceutical and tech investments, and Kary Mullis certainly did say that Fauci is a non-scientist and bureaucratic idiot who, he predicted, would work with the WHO and CDC to use PCR testing to create a panic over a new pandemic, using the model they stumbled upon which generated massive profits from the public purse when rogue cancer researchers managed to convince the world of the terrors of HIV.
Alison says:
Ladies & gentlemen, I rest my case. A Gish gallop par excellence.
Michael Crowe says:
Hmm first you replied in minutes and now .. crickets. Seems our dialog mutated into a monolog. Perhaps I’m blocked and invisible to you now. It’s liberating. Talking into thin air. I’m free to address the elephant in the room. Which is financial motive. You see, we all have one, almost always, because our world is entombed in materials technology and chemistry and mired in false charity and permeated by fear. Biology is not any of that. It’s life and it’s cumulative and it’s a good time despite the suburbanites and their tracts. But the Huxley model merged with the huckster model and molded your mind in the image of a maker who is not your self and you are lost and know not what to say
Over. Out.
Alison says:
Hmm first you replied in minutes and now .. crickets. Seems our dialog mutated into a monolog
Michael, you’re in Canada. I’m in New Zealand. Check the time zones & maybe try not to be such a silly person.
Since it’s clear from the rest of your “monolog” that you’re at the very least flirting with germ theory denial, a creationist, and a confirmed Gish galloped, I’ve no intention of engaging with you further. Your existing comments will remain, so that others can see what I mean, but anything further from you will be consigned to the spam folder.
Alison says:
Sorry, Anabel – I’m not providing you with a platform to slander others. Your comment has gone where it belongs – into the trash.
Ray Cattini says:
So is Kary Mullis wrong about his own invention, PCR, when he says its not a clinically diagnostic test and cannot be used to determine whether someone is infectious?
Alison says:
His own patent for PCR states quite clearly that it can be used as a diagnostic test for the presence of pathogens. Mullis only started saying it wasn’t when he became an HIV/AIDS denialist.
This is easily confirmed & in fact I’ve blogged it.
Tom West says:
Alison; Thank You, Thank You…..Thank You!
Roy McIntosh says:
WHO??? Yes who is all behind the covid shenanigans. Pulling the strings from the back ground. We see advisors to Sturgeon/Johnson/Merkel/Macron all have links in one way or another to Gates! But is he just one of many and can the Banks/Great Reset/Satan GATES Cult/Royals/Rothchilds all be behind the sinister times??
WHAT??? Is all behind it! We have heard a lot about build back better/New normal/You shall own nothing but be happy!??? The Johnsons and GATES have openly spoken about depopulation and I think even Satan GATES mentioned vaccine!?!?!? This has not just happened on an evil minutes thinking this has all been planned as you can see there is total control over cops/media/health services/councils etc so it is long term evil plans being rolled out!
BONUS POINT!!! How many were killed by blanket DNR and the wide usage of MIDAZOLAM??? How many have died and still dying from wilful neglect from the NHS???? Then along comes the SYNTHETIC PATHOGEN injections and how many thousands has that killed and how many hundreds of thousands of adverse reactions???? Are doctors falsifying health reports and death certificates to keep the numbers lower than what they are???? I asked the MHRA if the injections contained GRAPHENE OXIDE and they replied NO!?!? So what is causing the blood clots/heart problems/extreme shaking etc if not GRAPHENE OXIDE. There has been enough cases reported so surely an investigation of some sort would have been carried out but it seems not as the injuries and killings continue!????———————
—————————————-
Now I have forwarded information and my thought on the matters to various bodies and I stand by what I have said!? I have openly said that the politicians and NHS should be on murder charges for the killing of thousands of elderly!? Cops/media/councils etc should also be on criminal charges of one order or another for the bullying and scaremongering as it has been the action of evil gestapo! I am sure there shall be families/friends of people that have died or been injured by the injections looking to take legal action????
Alison says:
This is an NZ blog, Roy; your tirade against the NHS isn’t relevant here. You appear to have been misled by the nonsense pushed by Sheri Tenpenny et al, given your comments on graphene oxide. Bonus points for the Godwin in your final paragraph.
Chris says:
I have just read all this and as a result have a greater understanding of the issues raised.
Thank you Alison for taking the time to enlighten us all from your knowledge.
I feel a lot of these questions have had to be asked and I feel more informed and know where to look further.
It is not easy times for any of us and we need to look at what is important to us all.
It has something to do with friends and family, realising our potential and that of those around us.
We have a chance here to find solutions using the higher realms of our nature as humans.
I challenge you all to do this. Cheers Chris
Alison says:
Thanks, Chris; I’m glad you’ve found the post & comments thread helpful.
Paula says:
Hi Allison, thanks for your full explanations. Being the creator of the PCR test why wouldn’t Mullis fully comprehend the use of it?
His credentials would indicate when PCR testing is reliable and should or should not be implemented and relied on?
Why can’t he change his thinking on how it can be used? When further information comes to hand hopefully that’s what one would do….
Robert Malone who co-invented mRNA vaccines while working with the Salk Institute is raising alarm about current vaccines and warning that the spike protein is potentially harmful. Yet he is silenced. Healthy debate would be extremely helpful.
Alison says:
Mullis didn’t change his mind when more data became available; he changed it when he got into HIV/AIDS denial. (Its also worth remembering that he wasn’t the sole inventor but one of several, & none of the others have made the same claim.)
Malone’s claims are all over the place; he’s hardly being silenced. It’s a bit of a stretch to claim he invented mRNA vaccines: https://www.logically.ai/factchecks/library/3aa2eefd
Alison says:
We also need to remember that PCR is used in a very wide range of applications: determining the presence of pathogens, yes, but also forensic investigations, aDNA research (including into our own species & its relationships with near relatives), cloning… (eg https://pubmed.ncbi.nlm.nih.gov/7580841). At this point it doesn’t really matter what Mullis might have thought.
Richard says:
Hello Alison
Kary Mullis didn’t become an AIDS “denier” He became sceptical that the HIV virus was the sole causative agent of AIDS. He wrote a paper that he wanted to reference with appropriate scientific literature that proved the hypothesis that HIV causes AIDS, and he couldn’t find it! He even asked Luc Montagnier and he didn’t know either.
On the subject of PCR. The FDA released this document https://www.fda.gov/media/134922/download On page 40 it states “Since no quantified virus isolates of the 2019-nCoV were available for CDC use at the time the test was developed and this study conducted, assays designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA (N gene; GenBank accession: MN908947.2) of known titer (RNA copies/µL) spiked into a diluent consisting of a suspension of human A549 cells and viral transport medium (VTM) to mimic clinical specimen”
Do you have any scientific literature that shows that a “quantified” virus isolate has been used to confirm the accuracy of the tests before they were put into use? If not, is it possible that the tests are picking up particles that were used in the “Mimic”?
Other interesting things this document says are,
• This test cannot rule out diseases caused by other bacterial or viral pathogens.
• Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms.
• The performance of this test has not been established for monitoring treatment of 2019-nCoV infection.
• Positive and negative predictive values are highly dependent on prevalence. False-negative test results are more likely when prevalence of disease is high. False-positive test results are more likely when prevalence is moderate to low.
• Inhibitors or other types of interference may produce a false-negative result. An interference study evaluating the effect of common cold medications was not performed.
I agree with your statement regarding the fact that Dr Bailey is also promoting a book. This doesn’t help her cause. But it is certainly healthy to be sceptical, after all that is what science should be about.
It seems that science is more about “consensus” and “grants” and less about objective rigorous debate based on what the empirical evidence says.
Alison says:
It seems that while Mullis was unable to find the evidence he wanted, others were able to do so. For example, this summary/retrospective by Robert Gallo. https://retrovirology.biomedcentral.com/articles/10.1186/1742-4690-3-72
If not, is it possible that the tests are picking up particles that were used in the “Mimic”?
Since the “mimic” was an RNA sequence from the virus (https://www.ncbi.nlm.nih.gov/nuccore/MN908947.2) then the tests are picking up the viral genome.
This test cannot rule out diseases caused by other bacterial or viral pathogens. – well, of course it can’t; all it’s doing is testing for the presence of SARS-Cov-2. Other tests would be needed to confirm or deny the presence of other pathogens.
Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms. – which is why the report generated by each test includes the CT number.
The performance of this test has not been established for monitoring treatment of 2019-nCoV infection. And your point would be?
Karla Winston says:
Alison says:
August 4, 2021 at 2:56 pm
It seems that while Mullis was unable to find the evidence he wanted, others were able to do so. For example, this summary/retrospective by Robert Gallo. https://retrovirology.biomedcentral.com/articles/10.1186/1742-4690-3-72
Jon Cohen says:
HHS: Gallo Guilty of Misconduct
https://www.sciencemag.org/site/feature/data/aids2002/pdfs/259-5092-168.pdf
Kary Mullis says:
Gallo is a liar.
00:44:26
https://odysee.com/@I-Rabbi-T:3/-Kary-Mullis–PCR-Inventor—-The-Full-Interview-by-Gary-Null–HIV-AIDS—(1996):b
How do you respond to these arguments Alison? Thank you for keeping everyone informed!
Alison says:
Well, they aren’t really arguments. The fact that Gallo was found guilty of misconduct back in 1993 doesn’t automatically mean that the retrospective I cited is incorrect or irrelevant (especially because it’s supported by other sources).
And seriously? An interview from 1996 with Gary Null, of all people? https://en.wikipedia.org/wiki/Gary_Null
Michelle says:
Love your work Allison!
Chris S says:
I’ve had correspondence with the CDC, I’ve written the WHO, read the primary virology papers, I’ve spoken to a tremendous number of Dr.s, Scientists, and whole bunch of regular folks alike and not one person or organization has been able to present even ONE scientific study where they’ve done ANY of the things below:
(1) Purified/Separated out a real life “virus” from someone.
(2) Scientifically demonstrated that these virus particles were the likely cause of any disease.
(3) Used proper scientific control experiments. Meaning they scientifically compared fluid samples from a “Healthy” person against those from an “Infected” person, with all methods and procedures being equal in the experiments.
(4) Validated the PCR test against a purified out virus (the necessary Gold Standard needed to validate any test like this)
(5) Followed the Scientific Method.
Do we see the problem here?
If you know of even a SINGLE study where ANY of the things above where done I’d genuinely like to see it.
Alison says:
In response to your first item: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7045880/
How SARS-Cov-2 causes disease: https://science.sciencemag.org/content/369/6503/510.summary
James True says:
Alison, the paper you referenced by Kim is address directly by Bailey. Maybe you didn’t absorb her position fully? Kim was contacted and explained they did not isolate from a pure sample either. Hope you caught that.
Alison says:
All viruses have to be grown in cell culture prior to isolating them. Bailey’s questions to various researchers were so phrased as to induce a “no” answer.
James says:
Isolating a virus can mean three different things depending on which lab you ask. This problem is addressed and by Dr Racinello and many others. Sounds like you took the word isolated to mean, we found the virus inside a human cell and separated it from the cell and removed the RNA from the virus center. But none of that happened.
Also, Dr Bailey did not ask “yes or no, did you isolate and purify the virus “ lol. She asked for details on what they meant by isolated and clarified by asking if it was purified. Not one of the covid samples was isolated from a pure sample.
Alison says:
I know exactly what she asked – I’ve included a screenshot of her question in this post. That question is deliberately worded in a way that elicits a “no” response.
Petra Liverani says:
I wonder what your response would be, Alison, to Sam Bailey’s recent video, Once Upon a time in Wuhan. Have you watched it?
https://odysee.com/@drsambailey:c/Once-Upon-A-Time-in-Wuhan-Odysee-Exclusive-Comp:2
Alison says:
I’ve watched enough of Bailey’s material already to know that it contains a lot of misinformation & misdirection. I doubt there’d be anything different in this one, to be honest.
John McMahon says:
Thank you so much for taking the time to refute this non sense on youtube. While reasonably well educated (currently pursing my masters, but not in biology) I don’t have the background to sift the fact from the fraud or misrepresentation but I suspected something wasn’t correct considering I saw this youtube post from an anti-term theory facebook group. Researchers like yourself should be commended for taking the time to refute these types of posts on social media. Sadly because these types of post are sprinkled with medical jargon and created by someone who obviously has some education it is hard for a lay person to know what is accurate and what isn’t; and lets be honest most won’t dig a little deeper to fact check since these posts agree with their world view 🙁
Alison says:
Thanks, John – glad you found the post useful.
a says:
How tragic this is: you don’t have the background to sift the fact from the fraud or misrepresentation but you still post a comment taking sides based on nothing but “suspicion”. Gosh, what a time waster! She didn’t “obviously has some education”. She is a DOCTOR! And knows
exactly what she is talking about.
Alison says:
Dr Bailey is a GP who specialised in surgery, as far as I know. That is, she’s not an immunologist, epidemiologist, or virologist & it’s clear – just from this one video – that on those subjects she does not know “exactly what she is talking about”. (If she did, she wouldn’t keep banging on about culture & isolation of bacteria when SARS-Cov-2 is a virus, for example.)
Ken Francis says:
Add my kudos Alison; great to see knowledgeable and sane reasoned rebuttals to this spurious rubbish. As someone on one of Prof Raciniello’s excellent TWIV videos recently observed, the unvaccinated are about to become the control group as they sadly now dominate the hospitalisation and death stats.
So thanks!. Cheers from over the pond in Sydney
a says:
https://www.beckershospitalreview.com/public-health/nearly-60-of-hospitalized-covid-19-patients-in-israel-fully-vaccinated-study-finds.html
Alison says:
This is more nuanced than I suspect you’d like the reader to think, given that there are multiple confounders in play: https://www.covid-datascience.com/post/israeli-data-how-can-efficacy-vs-severe-disease-be-strong-when-60-of-hospitalized-are-vaccinated
John Duval says:
“Remember that covid-19 was first identified as a distinct infection back in December 2019”
> No it wasn’t. There are no unique features to Covid-19. A cough is a cough, a fever is a fever, pneumonia is pneumonia, and no symptoms are no symptoms.
“The viral genome was described – and shared globally – a little earlier, in mid-January that year.”
> No that was the genome of SARS1, tweaked. The fact that you even say this sort of silly thing at the outset, tells us your whole basis is wrong and that therefore what follows in your critique is flawed.
“And there have been a large number of papers describing isolation and genomic sequencing from patients the world over (for some examples see here, here, here & here).”
> No those papers illustrate the very thing Sam has refuted. They are using the term “isolate” on an a-priori basis: they are presuming what they are seeing is viruses and then declaring them to be isolated. That is called “begging the question”.
“And here’s a detailed description of steps taken to grow & isolate the virus.”
> And no, it isn’t. It’s exactly the same thing that Sam has refuted, again.
Your arguments are circular. You’re good at disguising your circularity, but not good enough.
Alison says:
No it wasn’t. There are no unique features to Covid-19. A cough is a cough, a fever is a fever, pneumonia is pneumonia, and no symptoms are no symptoms. -and your qualifications to make these distinctions are what, exactly?
No that was the genome of SARS1, tweaked. – that is simply BS.
No those papers illustrate the very thing Sam has refuted. They are using the term “isolate” on an a-priori basis: they are presuming what they are seeing is viruses and then declaring them to be isolated. – that is not how viral isolation works. Heck, I’ve even linked to explanations – although I note that you claim that somehow the virologists who wrote that are wrong & that not-a-virologist-Bailey is correct.
Guy says:
Thanks for fact-checking Sam Bailey. I know people who quote her and when I find evidence-based refutations for her out-of-context quotes, they appeal to her ‘authority’ as if facts require a degree. Sadly the more I refute the misinformation, the deeper these people search for the ‘truth’.
Keep up the good work 🙂
James True says:
It’s concerning in the very first paragraph you claim she doesn’t reference or address any studies but almost all of her videos including this one are her rebuttal of a paper which she links in the description. Yet you, debunking her, will not link her video in your description. Why?
Alison says:
Because I see no reason to give her financial support (directing hits to her videos & bumping up advertising revenue), or to direct others to her misinformation.
Ellen White says:
Who is Alison and what are her qualifications? If she is Alison Jolley she has a background in geoscience and education. Great. Are there conflicts of interest here where she is moving way out of her field? We have seen in this ‘debate’ digital trillionaires, sports people, beaurocrats etc being ‘experts’. I think this is far too important an issue with the vaccination injuries which are accumulating (CDC website amongst others) as well as the economic devastation which has been brought about to have trolling as the main method of debate.
Alison says:
It’s very easy indeed to find out who I am via the University’s website. But for the record, I have a biological sciences PhD.
Rooibos says:
Hi Alison,
I have checked your LinkedIn and only PhD I can see is Doctor of Philosophy, please clarify.
Also according to FDA website, phase IV is not just for monitor effectiveness as you stated, please, omitting critical information doesn’t help in my humble opinion.
“Although the vaccine development process and FDA’s evaluation are rigorous and comprehensive, there is still a need for ongoing surveillance of vaccines after FDA-approval to identify uncommon adverse events or long-term complications that may occur, and sometimes to monitor effectiveness. In certain cases, the FDA may require the manufacturer to conduct post-marketing studies to further assess known or potential serious risks. (These studies are sometimes called Phase 4 of development).”
Maybe claims still proceed?
Alison says:
In NZ – & in many other countries – the Doctor of Philosophy (PhD) is the highest research qualification you can earn via enrolment & completion of a research program at university. (The Doctor of Education & Doctor of Laws are the equivalent.) Mine is in biological sciences.
Pfizer/BioNTech stated that they would continue to monitor participants after phase III ended to determine the longevity of the immune response. Your statement from the FDA website applies to all vaccines & is ongoing for all vaccines currently licensed.
Alison says:
By the way, I’m not on LinkedIn, so I have no idea which Alison Campbell you looked up.
Christian says:
As a doctor in a developing country that is ravaged by this disease and have personally seen the effects it has on our patients, family, and friends; I am grateful for stumbling upon your blog. There has been a growing virus denialist movement in my country that have been using these very same talking points.. and it has been frustrating, trying to eloquently explain how wrong those talking points are to non-medical people.. I have been called brainwashed and/or indoctrinated with “western mainstream medicine” by people with absolutely no medical training and only reference videos like hers.. This will help me try to show people counterpoints to all these quackery being referenced on the internet.. Thank you for doing the work and for the references..
Alison says:
Thank you – I’m glad to hear this post’s been helpful for you. And I’m really sorry to hear that you’ve been attacked for your science- & evidence-based approach.
John says:
Hi Alison, Full transparency I am a lay person from Australia, with no scientific background. I don’t want to be disrespectful to you or your expertise in the field, but I’m just looking for truthful unbiased answers, it sounds like you have the knowledge hence my questions below that i hope you can answer.
I am glad you are challenging Sam Bailey, and I’m glad Sam Bailey is challenging the narrative, to be transparent I enjoy watching her videos and to the Layperson like me, she seems to poke some holes in the mainstream narrative, which is healthy because when you are not allowed to challenge the narrative it makes people like me even more intrigued and skeptical about what is really going on.
So while in lockdown and having nothing better to do because I can’t work due to a deadly virus, and with my basic lay person skills I come across this article https://wwwnc.cdc.gov/eid/article/26/6/20-0516_article#r1 and I’m trying to understand how they separated the (SARS-CoV-2), not believing Sam and not believing the mainstream narrative I would like to understand why there is an argument? Why can nobody give a good enough answer to put the question of isolation to rest?
The lay person that I am, if I have a bucket full of screws I can pull one screw out of the bucket and run tests on it, from this article I don’t see how they isolated one screw from the bucket of screws?
Once again in my lay terminology, it seems like they are extracting a bunch of screws out of someone’s nose, mixing it with some bolts from monkey kidneys in a bucket, mixing gently with a pipet then running the PCR test to verify if the screw we are looking for is in this mix of screws and bolts that we created?
If all the screws are mixed up with bolts and the screws and bolts are different sizes different shapes etc, how do you know that:
– The pcr test is picking up the particular screw you are searching for?
– How do you match the visual appearance of the screw with the PCR test result
– How do we know that that screw is in fact causing the illness? Has this screw been separated and caused illness in a human?
– If we are using genetic sequences from a database to determine if they have found a new type of screw, yet not separated that screw from the bucket, how did they obtain the genetic sequence in the database? They would have had to isolate something in the past to create the original genome sequence?
– At some point in the history of the coronavirus someone must have isolated the virus in order to create these genome sequences? You can’t look for a screw in a bucket of screws and bolts without first knowing what you are looking for?
– Who found the first coronavirus?
– Who determined the first genome of the coronavirus?
– How did they isolate the first coronavirus so that they could determine the genome?
From the article they use very specific and very detailed descriptive language like:
“We scraped infected Vero cells from the flask”
“we pipetted 50 μL of serum-free DMEM”
“mixed gently by pipetting”
“we scraped cell monolayers with the back of a pipette tip”
To the moran like me, these statements above sound very descriptive, detailed, mechanical and crude when dealing with a virus that is nM in size, how does it help me that they mixed gently with a pipet, yet fail to describe to me how you separated SARSCOV2, if they can use the above descriptive language I cant seem to find the descriptive language explaining how they separated the screw from my hypothetical bucket of screws, I feel like they are running tests on a bunch of stuff.
I want to be proven wrong, I don’t want to believe that this is a scam, but nobody is answering the questions well enough to silence the likes of Sam Bailey and the other professionals that seem to be questioning the narrative also.
Can you explain it in language that a lay person like me can understand so I can spread your explanation to the rest of the people that seem to be questioning everything like me?
Not all of us are scientists but to silence the sceptics like me we need some lay language to quell our questions.
Hopefully, you can set me straight. Happy to take the discussion offline if you prefer. But this post is from a lay person representing the Lay people of the world.
John says:
Hello Alison,
Do you know if any covid 19 viral culture experiment where a control experiment was conducted to see if cytopathic effects are the result of covid 19 or due to the conditions of the experiment where antibiotics where added to the culture. Dr Sam bailey mentioned that mock cultures are sometimes shown in journal articles showing no cytopathic effect but she questioned where in the methods section is this discussed so we the readers can know how the culture was generated. She also mentioned that Dr Lanka conducted a covid 19 viral culture experiment and showed that cytopathic effects were similar in the control experiment. Proving that the conditions of the experiment such as adding antibiotics caused CPE. If you have a link to an article where I can read the method section for a control experiment that would be helpful to clear up this issue
Alison says:
There are quite a few papers that describe their methods; here’s one: https://journals.asm.org/doi/full/10.1128/JVI.02304-20 – it might also be helpful to review how a virus’s replication cycle damages cells: https://courses.lumenlearning.com/biology2xmaster/chapter/virus-infections-and-hosts
This Stefan Lanka? https://time.com/3743883/german-biologist-measles-pay/ Given he seems inclined to deny the existence of viruses (as does Sam Bailey, in her book), I think I’d prefer to get advice from the mainstream community of research virologists.
John says:
Thanks Alison for the links, I was wondering if you could look at a paper that Dr.
Cowan and Dr. Lanka referred to by Enders called “Propagation in tissue cultures of cytopathogenic agents from patients with measles”
They use this quote in this paper to say when a control experiment was conducted by Enders he couldn’t distinguish CPEs from cultures infected with measles:
“A second agent was obtained from an uninoculated culture of monkey kidney cells. The cytopathic changes it induced in the unstained preparations could not be distinguished with confidence from the viruses isolated from measles”
I was wondering what are your thoughts on this quote?
Alison says:
Lanka again? John, that paper was written in 1954. Technology has come a long long way since then. Anyone citing it today in support of a claim that viruses (in general or particular) don’t exist is being disingenuous in the extreme (& that’s being polite).
John says:
Hi Alison, I tried reading the article but I need a subscription. I was wondering if you had access to it. I know in the next sentence Enders says however and says something about staining. I know it is an old article but this paper won him the Nobel prize. Enders is the father of virology and his viral culture experiment is still used today. If you could debunk this idea it would be helpful.
Alison says:
He & Peebles used staining to identify chromatin in their culture cells & to visualise the cells overall. As I said, technology has moved on since then; SEM & TEM were in the early phases of development then, plus molecular biology technologies had hardly begun development. However, these researchers were satisfied that they had identified measles. This is their conclusion:
Conclusion and Summary
The findings just summarized support the presumption that this group of agents is composed of representatives of the viral species responsible for measles.
Eight agents exhibiting the properties of viruses have been isolated in cultures of human or simian renal cells from the blood or throat washings of five cases of typical measles. Multiplication of the agents in vitro is accompanied by characteristic changes in the cells. Primarily these changes consist in the formation of syncytial giant cells wherein the chromatin assumes a marginal position and is replaced centrally by an acidophilic substance of unknown nature. The cytopathogenic effect of at least one of the agents is inhibited by convalescent phase measles sera from other patients with measles. Antigen appears during cultivation in vitro of the measles agents that reacts specifically in complement fixation tests with convalescent phase measles sera.
Please note that the paper we’re discussing did NOT win him the Nobel Prize: https://www.nobelprize.org/prizes/medicine/1954/summary The prize was awarded for research into polio, not measles.
Incidentally, Lanka’s claims about antibiotics are almost certainly a red herring. Antibiotics are routinely used in cell cultures to keep the cells alive by eliminating/preventing bacterial contamination.
Grant Jacobs says:
For non-scientists like yourself this little video of SARS-CoV-2, the virus that causes COVID-19, infecting brain cells in bats, triggering cell fusion and cell death (cytotoxic effect) is probably more useful. Nothing like a simple visual recording of it doing the deed—killing cells—to make the point!:
https://www.nikonsmallworld.com/galleries/2021-small-world-in-motion-competition/sars-cov-2-infection-triggering-cell-fusion-and-cell-death-in-bat-brain-cells
(Recorded by virologists at the Institut Pasteur, Department of Virology in Paris, France.)
Richard says:
Hi Grant
as impressive as that video is there is still one important factor that you didn’t mention.
“Bats ultimately don’t get sick.”
Having a video like that where the”virus” is doing the same thing to human lung epithelial cells would be interesting!
Grant Jacobs says:
“But, but” is trying to resist – better to jump in and learn 😉
You asked for evidence of cytotoxic effects, you’ve seen that now. It’s there, right in front of your eyes 🙂 There’s plenty of more sophisticated evidence, but your lot seem to like videos as evidence, so it seemed the obvious choice.
Whether the animal gets sick or not doesn’t make that SAR-CoV-2 causes cytotoxic effects go away.
This little article might help you – in most cells in bats the virus usually has to leave cells in order to get into new ones, which exposes the virus to the bat’s immune system. In humans the virus is less often exposed because to some extent the virus can go directly into neighbouring cells. But in both there is cell death – the cytotoxic effect you asked about. https://www.nytimes.com/2021/08/22/science/microscopic-bat-brain-virus.html
For what it’s worth — while people often refer to the bats ability to carry viruses as a “win”, it’s just as equally a failing—they can’t get rid of the viruses like most mammals can. They stuck with them, fighting out an ongoing battle to keep the viruses suppressed enough to not infect vulnerable parts of their bodies.
Alison says:
It’s also been shown in vitro, using some rather cool work with 2D organoids: Mart M. Lamers, Jelte van der Vaart, Kèvin Knoops, Samra Riesebosch, Tim I. Breugem, Anna Z. Mykytyn, Joep Beumer, Debby Schipper, Karel Bezstarosti, Charlotte D. Koopman, Nathalie Groen, Raimond B.G. Ravelli, Hans Q. Duimel, Jeroen A.A. Demmers, Georges M.G.M. Verjans, Marion P.G. Koopmans, Mauro J. Muraro, Peter J. Peters, Hans Clevers, Bart L. Haagmans. An Organoid‐derived Bronchioalveolar Model for SARS‐CoV‐2 Infection of Human Alveolar‐type II‐like Cells. The EMBO Journal, 2020; DOI: 10.15252/embj.2020105912
Richard says:
Don’t you mean cytopathic effect?
Alison says:
No, Rob, you don’t get to spew your conspiracy-theory antivax nonsense, making claims which indicate you don’t understand the technology you’re dissing, in the comments section on this post.